
Medicare Outpatient Code Editor (OCE) and 2025 UpDates

See how the NOPAIN Act Impacted the Outpatient Prospective Payment System
January 2025 saw 168 new Level II Healthcare Common Procedure Codes (HCPCS codes) integrated into the Medicare Outpatient Code Editor (OCE) and 2 new Outpatient Prospective Payment System (OPPS) Status indicators. New legislation had an impact on this years OPPS.
Medicare employs the Integrated OCE (I/OCE) program to process claims for all outpatient institutional providers, including hospitals that are both subject to the OPPS payment and not subject to OPPS payment. Claims are identified in the electronic claim record as either 1= OPPS or 2 =Non-OPPS, and a blank or zero or any other value defaults to 1.
There are 3 main functions of the I/OCE, and they are as follows: Assign an Ambulatory Payment Classification (APC) number for each billed service covered under the OPPS, and return information for use by the “pricer system”. Second it edits the electronic claims data identifying errors by raising a unique flag for each edit. Lastly it assigns an APC payment group for services submitted on the electronic claims by a select group of Non-OPPS hospitals.
Each electronic claim supplies the (header/demographic) data, plus all services provided (line items). The I/OCE is limited to review of a single claim and does not have any cross claim capabilities, it can accept up to 450 lines per claim. The I/OCE orders the line items by date of service and then identifies each individual error with a list of edit numbers and the associated actions that are required for correction. The I/OCE functions require the system to be up to date with LEVEL I and II HCPCS codes/modifiers, and ICD-10-CM diagnosis codes in order to apply specific logic to the codes for edits. It is updated and released quarterly.
When the I/OCE software processes a claim, the software provides the following:
Edits a claim for accuracy of submitted data
Assigns APCs
Assigns CMS-designated status indicators
Assigns payment indicators
Computes discounts, if applicable
Determines a claim disposition based on generated edits
Determines if packaging is applicable
Determines payment adjustment, if applicable
The 2025 OPPS final rule included policies that align with several key goals of “the Biden-Harris Administration, including responding to the maternal health crisis, addressing health disparities, expanding access to behavioral health care, improving transparency in the health system, and promoting safe, effective, and patient-centered care.”
One example of this is the bipartisan NOPAIN Act, which was passed and went live on January 1, 2025. This was designed to increase patient and provider access to non-opioid pain management options in the ASC and Outpatient surgery arenas by removing the barriers associated with reimbursement for the Medicare population. In order to facilitate this, 2 new status indicators (SI) were introduced to the OPPS to identify non-opioid drugs and biologicals and non-opioid devices. Under the OPPS, non-opioid drugs and biologicals under this policy, will be assigned a status indicator of K1, while non-opioid devices would be assigned a status indicator of H1.
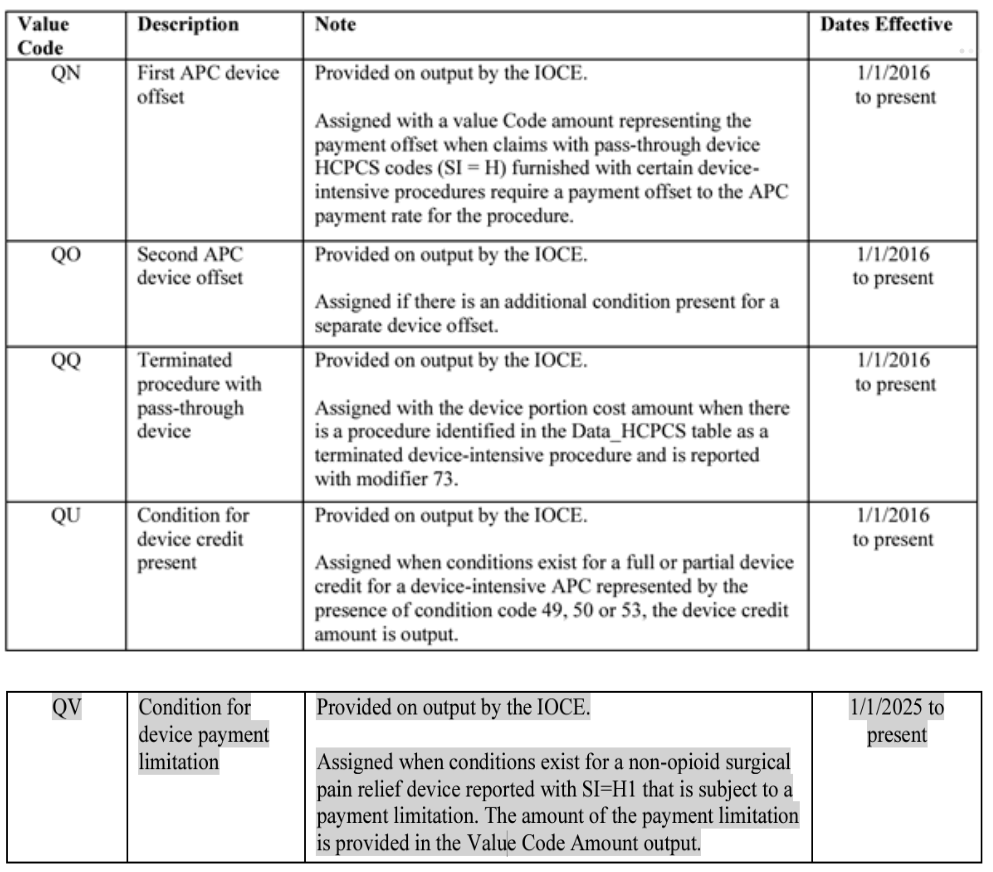
5.8.4 Payer Value Codes for Device Intensive Procedure Processing for Payment Offset or Limitation

Device HCPCS provided for non-opioid related post-surgical pain relief are identified with SI=H1 and are subject to additional claims processing. According to the OCE update 5.8.3: “device HCPCS with SI=H1 are not subject to payment offset, and instead, are subject to a payment limitation based on a CMS defined percentage of costs for the surgical procedure. When a device HCPCS with SI=H1 is reported appropriately with a surgical procedure requiring the device, the IOCE provides payer Value Code QV with a Value Code amount representing the amount of the payment limitation for the device HCPCS. When the non-opioid device is not reported with an appropriate surgical procedure, or any other OPPS payable procedure (SI = J1, J2, P, Q1, Q2, Q3, R, S, T, U, V), the claim is returned to the provider (edit 98). In the unlikely event there is more than one non-opioid device present, the payment limitations for each device are summed and the total amount is placed in the Value Code QV Value Code amount.”
5.8.4 Payer Value Codes for Device Intensive Procedure Processing for Payment Offset or Limitation
Another piece of interesting legislature coming in 2026 is notable for the fact calendar year 2025 is the final year of the add-on payment for Tc-99m when the Tc-99m is produced without the use of HEU, as the Secretaries of the U.S. Departments of Energy and of Health and Human Services have issued a certification that there is sufficient global supply of Tc-99m without the use of HEU available to meet the needs of patients in the United States.
CMS is finalizing a proposal to address the payment inequity in this rule by establishing a new add-on payment, of $10 per dose, for radiopharmaceuticals that use Tc-99m derived from domestically produced Mo-99, starting on January 1, 2026. They indicated the $10 add-on payment for domestically produced Tc-99m would ensure equitable payments, by paying providers who use domestically produced Tc-99m radiopharmaceuticals, when available, an amount that reflects the anticipated higher cost of these products.
Please see the references below for the full list of 2025 OPPS changes to the I/OCE.
References
https://www.cms.gov/medicare/coding-billing/outpatient-code-editor-oce/quarterly-release-files
https://www.cms.gov/medicare/coding-billing/outpatient-code-editor
ELEVATE MEDICAL SOLUTIONS: YOUR TRUSTED PARTNER MEDICAL CODING
At Elevate, we’re dedicated to helping medical coders like you excel. Stay ahead of the curve by subscribing to our blog for the latest resources, industry insights, and exclusive webinars where you can earn AHIMA-approved CEUs—all for free.
Join Our Community Today!