
Telemedicine in 2025

Changes and Challenges
Navigating the new and complex Telehealth landscape in 2025 is challenging. There were unprecedented changes at the end of the Public Health Emergency (PHE) on May 11 of 2023. Now many Telehealth benefits are set to expire on March 31, 2025.
The Coronavirus Aid, Relief, and Economic Security Act and the Public Health Emergency (PHE) protocols were enacted in 2020 to maintain access to healthcare during the COVID 19 pandemic. These policies allowed for the following:
Allowances for providers to offer care across state borders regardless of licensure
Reimbursement for telemedicine equivalent to that of in-person visits,
Relaxation of HIPAA (Health Insurance Portability and Accountability Act) compliance requirements,
New protocols and ICD-10 (International Statistical Classification of Diseases, Tenth Revision) codes for telemedicine visits
Permission to prescribe certain controlled substances via telemedicine,
promotion of telemedicine expansion for Medicare,
Medicare Matters MM13887 for Transmittal number R12975CP cited the following: “Telehealth Services Absent Congressional action, beginning January 1, 2025, the statutory limitations that were in place for Medicare telehealth services prior to the COVID-19 Public Health Emergency will retake effect for most telehealth services. These include geographic and location restrictions on where the services are provided, and limitations on the scope of practitioners who can provide Medicare telehealth services.” The list of approved Telehealth services for 2025 can be found at https://www.cms.gov/Medicare/Medicare-GeneralInformation/Telehealth/Telehealth-Codes.
The final status of the Medicare Telehealth Policies for 2025 allows for a one year extension for the following services:
Virtual direct supervision,
Teaching physicians can supervise residents virtually when the resident is providing a telehealth service,
There are no limits to the frequency of telehealth visits in the hospital or in a nursing home, and
There is no need for the provider to report their home address to Medicare.
There was also a permanent change to the definition of telecommunications systems to allow for audio only services. The clinician must still have the ability to provide audio and video services.
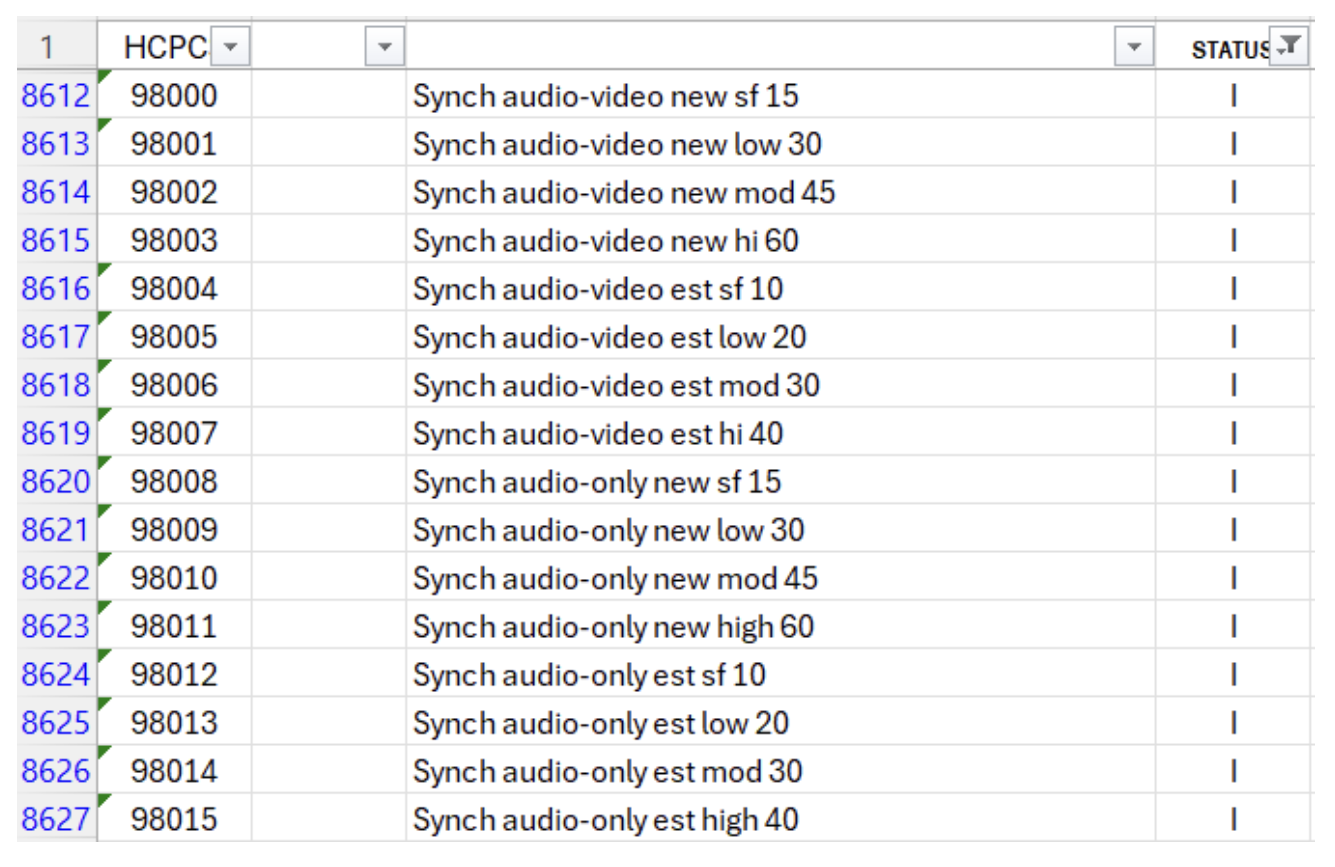
There are new telemedicine Current Procedural Terminology (CPT) codes (98008-98016) for synchronous, real time, interactive encounters between a physician of other qualified healthcare professionals and a patient using either an audio - only or a combined audio - visual telecommunication device. These services are based on the time spent or the level of medical decision making. These are not for use for brief follow-up calls from a prior encounter to report the findings of diagnostic tests. If performed on the same “date of service” as a face to face E/M service, then the time and MDM elements are bundled up into a single service. Coders need to pay close attention to the nuances in this new code set and the AMA guidelines under ►Telemedicine Services◄ in the 2025 CPT book. The new codes are divided into sub - groups based on the type of communication and whether the patient is new or established.
Synchronous Audio-Video Evaluation and Management Services for a New Patient code to 98000-98003and for an Established Patient use codes 98004-98007.
Synchronous Audio-Only Evaluation and Management Services for a New Patient code to 98008-98011 and for Established Patients use 98012-98015.
Brief Synchronous Communication Technology Service such as Virtual Check-In codes to 98016
Medicare has assigned a status indicator of “I” to these new telemedicine CPT codes, indicating they are not valid for Medicare purposes.
The FAQ for Telehealth on the CMS website indicated the correct way to code Telehealth is using POS 02 with the correct CPT code and modifier 95 or modifier 93. These modifiers are appended to the CPT or HCPCS code for a service that was conducted through real-time audio and video or audio only communication between a healthcare provider and a patient. Please see MLN901705.pdf and telehealth-faq-1-8-25-cmsd-ogc-1.14.pdf for more information.
The Telehealth service list has designations for permanent and provisional assigned to each code. In the CY 2024 PFS final rule (88 FR 78861 through 78866), CMS implemented a revised 5step process for making additions, deletions, and changes to the Medicare Telehealth Services List (5-step process). Calendar year 2025 Medicare Telehealth Services List shows the services are no longer categorized as “Category 1” or “Category 2,” each service is now assigned a “permanent” or “provisional” status. A service is assigned a “provisional” status if the available evidence does not yet demonstrate definitive clinical benefits from telemedicine visits, but they are included for further study. There is no time limitation for services designated as “provisional” on the Medicare Telehealth Services List. Provisional codes were not recategorized for 2025 because CMS plans to conduct a comprehensive evaluation of all Medicare telehealth services with provisional status. Services included on the Medicare Telehealth Services List with provisional status will remain on the list.
Telehealth provides a plethora of benefits and is a highly convenient avenue for patient care. The future of these services continues to evolve, and coders must remain vigilant.
ELEVATE MEDICAL SOLUTIONS: YOUR TRUSTED PARTNER MEDICAL CODING
At Elevate, we’re dedicated to helping medical coders like you excel. Stay ahead of the curve by subscribing to our blog for the latest resources, industry insights, and exclusive webinars where you can earn AHIMA-approved CEUs—all for free.
Join Our Community Today!